Gnathology is the branch of dentistry that studies and treats the chewing system under all anatomical-functional aspects. There is a close relationship between the correct contact between the two dental arches, the mandibular muscles and the cranio-mandibular bones. Gnathology deals precisely with studying and restoring the correct balance between these districts by solving the resulting symptoms. The common goal of gnathologists is the identification of the correct cranio-mandibular relationship, its maintenance and restoration.
Chewing is perfected thanks to the intervention of the temporomandibular joint and the neuromuscular system (Fig. 1). The TMJ is a double joint consisting of two joint heads (the glenoid cavity above and the mandibular condyle below) between which the disc or articular meniscus is interposed. The disc is in turn fixed to the joint heads by means of tendons. All movements of the jaw involve both joint heads in a different way at times. There are 4 muscles involved in joint movements: the masseter, the temporal, the external pterygoid and the internal pterygoid. The muscles intervene in the 4 types of movement that the jaw can perform: closing (and opening), protrusion (when the jaw moves forward), retrusion (the jaw backwards) and laterality (when the jaw moves to the right or left). Often there are anomalies in the functioning of this complex system, and craniomandibular disorders can arise, which require the intervention of a specialist.
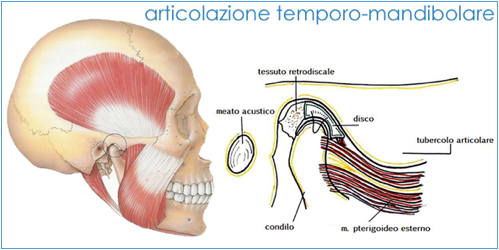
Fig. 1 – Temporo-mandibular joint
Cranio-mandibular disorders
Cranio-mandibular disorders (also referred to as temporomandibular dysfunctions of disorders or even myarthropathies) represent a category of different clinical problems involving some anatomical components of the masticatory system):
- The temporomandibular joint (TMJ)
- The facilities associated with the ATM
- The musculature
They can be divided into two large families:
- Intracapsular disorders are those disorders that mainly affect the joint. There are three main categories:
- Condyle-meniscal incoordination
- Structural alterations of the articular surfaces
- Inflammatory alterations
- Extracapsular disorders are those disorders attributable to a predominantly muscular component, that is to a functional hyperactivity of the masticatory muscle.
Causes
Currently, regarding cranio-mandibular disorders, we speak of multifactorial etiology, where the following causes can be recognized:
- Dental malocclusions: defects in contact between the teeth in the closing phase are considered predisposing or aggravating factors for cranio-mandibular disorders, especially in the case in which they cause a mandibular displacement, and therefore condylar, in the phase of maximum opening.
- Parafunctions: grinding or clenching of the teeth (bruxism is an example) are often associated with the etiology of craniomandibular disorders. The high intensity parafunction not only triggers pain, but also muscle fatigue, odontalgia, pain in the temporomandibular joint region, headache and even joint clicks.
- Posture: has a multiple role in the etiology of TMJ disorders. In fact, the vertebral column acts as a trait-union between the cephalic and breech districts.
- Psycho-social factors: it is clear that the emotional life of the patient, being the cause of parafunctions and also causing inadequate posture, is a determining factor in the etiology of these disorders.
- Other causes: at the base of this pathology there may also be bone fractures involving the mandible, the coronoid process and the condyle; or they can be linked to developmental anomalies (dysplasia, hypoplasia, hyperplasia).
What is important is to make the right diagnosis in order to set the correct therapy.
Symptomatology
Joint pathology can be completely asymptomatic or associated with symptoms of various kinds and degrees, depending more on the individual’s ability to adapt than on the degree of disorder.
Pain, especially in the chewing muscles and / or the joint itself, or radiated to the face, neck or shoulders is the most common symptom.
Other possible symptoms are:
- Movement limitations or “lock” of the jaw
- Joint noises such as clicking or roaring, even painful, when opening and closing the mouth
- Sudden change in dental occlusion: symptoms such as headaches, ear pain, dizziness and hearing problems can sometimes be linked to TMJ disorders.
Diagnosis
The clinical examination represents the first step towards the diagnosis of diseases affecting the joint system.
It includes:
- Inspection: must consider both the face and the oral cavity and must include a postural analysis of the patient that considers the alignment and body symmetry. It is important that the evaluation of the maximum opening of the mouth is performed (which must take place in a harmonious way, without jerks or deviations) and the protrusion and lateral functions.
- Palpation: it allows to discriminate patients suffering from joint pathology from those with muscular problems. By means of a digital examination in correspondence with the outermost portion of the acoustic meatus, the release of the condyle from the glenoid fossa in the opening movement of the mouth and any intra-articular showers can be appreciated. The palpation of the chewing muscles, which should always be symmetrical, must look for any overtones and contractures as well as the presence of “trigger-points”, a source of pain often referred to in the auricular, temporal and joint regions. Through the palpation of the preauricular region it is also possible to evoke pain in subjects with intra-articular inflammation.
- Auscultation: it can highlight the presence of two types of fundamental noises:
From this initial diagnosis, there are two types of joint “noises”:
- Pop or click type: clear, rapid, high-pitched noise, almost always and index of displacement and condyle-meniscal incoordination. If the snapping noise is present as an indication of disc dislocation, it almost always disappears causing the jaw to protrude; and the later its appearance in the opening movement of the mouth, the greater the anterior dislocation which the disc has encountered and therefore the greater the difficulty of its recapture and stable repositioning on the condyle.
- Type of rubbing or wet sand: low-pitched noise, prolonged throughout the mandibular movement, indicating a degenerative state of the joint heads (arthrosis).
There are also instrumental tests:
- The static and dynamic baropodometric (or stabilometric) platform, which is used to assess the patient’s body symmetry and overall postural structure.
- Electromyography, which aims to access a state of contracture or hypertonicity of the masticatory muscles and the influence that these may have had on the onset of joint painful symptoms.
Finally, the radiographic examinations to complete the diagnosis:
- Orthopantomography is useful as a screening technique to evaluate macroscopic bone changes, such as the length of the mandibular bone segments and their asymmetry, or a gross deformity of the condyles; it provides information on the number and state of the dental elements, but is not very suitable for the evaluation of joint alterations / pathologies.
- The TMJ stratigraphy must be individualized and is performed with mouth open and mouth closed, it gives information about the conformation and condylar excursion.
- Computed tomography (sagittal and coronal projection) offers much superior information to stratigraphy, albeit with higher costs. The CT accurately highlights the condylar morphology and in particular bone alterations due to osteoarthritis and asymmetries of the skeletal structure; however, it appears unsuitable in the diagnosis of intra-articular dysfunction since there is no clear representation of the meniscus, which can be confused with the external pterygoid tendon.
- MRI, performed with mouth closed and mouth open, in sagittal projection and coronal projection, is the main instrumental examination in TMJ diagnostic imaging. It also finds its indication in the examination of children and pregnant women, as it is non-invasive and free of radiological risks. The MRI allows to highlight in detail both the bone structures and the soft tissues and any intra-articular effusions. MRI is of great diagnostic value in cases of disc dislocation / dislocation of the disc, disc degeneration, osteoarthritis and in cases of inflammatory reaction of the synovium (Fig. 2).
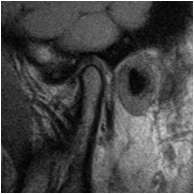
Fig.2 – MRI TMJ
- Kine-resonance or dynamic resonance is an even more complete and descriptive examination from the functional point of view of normal MRI. This examination gives us the possibility to visually check the joint movements and the alterations they undergo in cases of meniscal degeneration or dislocation.
- Arthroscopy is a more invasive method, which allows a direct view of the joint components, giving the possibility of diagnosing degenerative or inflammatory processes of the TMJ from the early stages, a very limited possibility with CT or MRI investigations., as well as diagnostic, above all therapeutic, as it allows the removal of intra-articular catabolites that is obtained with washing and also the “pump effect”, linked to the positive hydraulic pressure, causes a distension of the joint with possible consequent fragmentation of the adherent fimbriae, improving the mandibular function and obtaining a regression of the painful symptoms.
Therapy
Once the diagnosis has been made, the appropriate therapy is set up for the specific case. Furthermore, by virtue of the etiopathogenetic multifactoriality of craniomandibular disorders, the therapy related to this pathology appears to be varied, depending on the aspect that is considered predominant in its determinism.
The therapeutic approach, therefore, can be differentiated into:
- Symptomatic through drugs: consists in the prescription of drugs that act at the level of the muscles, favoring their relaxation. This type of therapy is indicated:
- In cases of muscle hypertonus linked to parafunctions, such as bruxism or clenching;
- In those patients in whom a hypertonic state of the masticatory and / or cervical muscles is noted on palpation.
- Pharmacological therapy can also be of the analgestic type, with the prescription of drugs that relieve painful symptoms, in cases of acute and disabling pain for the patient.
- Symptomatic using occlusal devices (bite, splint) (Fig. 3): used as a therapeutic aid for cranio-mandibular disorders, they are devices designed to stabilize an arch, as well as to generate a change in occlusal contact and muscle activity. In cases of disc dislocation, the construction of occlusal so-called repositioning devices may be useful, that is, which reposition the mandible in a more advanced position, in which the clicks normally present disappear.

Fig.3 – Bite
-
- Surgical-articular: they are particularly useful and necessary in cases of tumor pathologies, hypoplasia and hyperplasia, fractures, ankylosis, osteoarthritis and advanced arthritis, but they are also used as an aid in the reduction of painful symptoms in intra-articular disorders.
- Rehabilitation of occlusion: orthodontic, prosthetic and / or conservative are sometimes necessary exclusively, when the presence of certain pathogenetic factors is found in the occlusion, while at other times they are auxiliary to a more complex treatment or to prevent latent phase pathologies caused or aggravated by occlusal changes.
- Manual: it is particularly suitable for unlocking locking situations. In addition, physiotherapy of the masticatory and / or cervical muscles may be useful in some patients.
Furthermore, there are cases of multidisciplinary interest that require consultations with other specialists, such as:
- The otolaryngologist, for disorders of the vestibular and auricular apparatus;
- The ophthalmologist for changes in ocular convergence that affect the overall posture;
- The rheumatologist in patients in whom cranio-mandibular disorders are only a sign of a more widespread rheumatic pathology;
- The orthopedist when there are alterations and / or asymmetries of the spine, girdles or limbs;
- The neurologist when the pain symptoms are neuralgic or expression of headaches;
- The psychologist in patients where the involvement of the emotional sphere is predominant.
Posturology
From numerous studies in the literature, it has been seen that there are close correlations between TMJ disorders and posture.
Consequently, a TMJ disorder can have deleterious effects on posture and vice versa. We need remember that:
- The TMJ is a convex-concave and concave-convex joint between the condyle of the mandible, meniscus and temporal bone
- The muscles acting on the joint, called masticatory muscles, are masseter, temporal, internal and external pterygoid
- These muscles have the task of both stabilizing the joint and clenching the teeth (closing the teeth)
- Although these muscles are monoarticular, they can interact with all the other body muscles. Physical laws on complex systems have shown that when there are multiple forces acting on a system (the muscles on the skeleton) these forces are integral and interacting with each other.
- By (correct) posture we mean a correct skeletal joint succession regardless of the position of the body in space.
Connections between TMJ and Posture
Physiologically there should be no connection between TMJ and posture, but if the dentition is pathologically positioned this connection will take place. The most encountered events are three:
- Length difference between teeth (pre-contact)
- Excessive free space
- Decrease or absence of free space
Difference in length between the teeth (pre-contact): if in a dental arch there are teeth that are too short or long, during the closing movement of the mouth the chewing muscles will act asymmetrically (right-left) and with greater intensity to that physiologically necessary. The first consequence will be that the temporal condyle on the side of the “short” teeth must be positioned beyond the physiological position towards the mandibular fossa to allow contact. The jaw will thus have a torsive movement. Since there are many receptors within the mandibular fossa, this event can trigger painful symptoms mostly localized to the TMJ, ear and head. Furthermore, as explained in point 4 of the premises, the asymmetrical muscle activation in excess of intensity will determine the involvement of the other muscle groups starting from the neck muscles. Excessive intensity or muscular tension will not be limited only to the chewing muscles and therefore other joints will suffer the consequences of the pulling muscular forces, the cervical vertebrae will lose their symmetrical position, a shoulder can be elevated and if, the process will last over time, produce a complex series of skeletal alterations. In other words, there will be an alteration of the body posture.
Excessive free space: in a resting condition, i.e., with relaxed chewing muscles, the teeth should not be inn contact but have a “free space” of about 2 millimeters. This is the state of the brain that is believed to be restful and physiological. If the free space is excessive, for example for teeth that are “too short” overall, the chewing muscles should be permanently under tension to maintain a correct free space. To overcome this continuous effort, the muscular system and in particular the muscles located in front of the cervical spine, taking a fixed point on the third thoracic vertebra, move the entire head forward. In this way the dental arches come closer, releasing the work of the masticatory muscles. But bringing the head forward also means moving the body’s center of gravity. To avoid the loss of balance, the underlying muscle areas must be activated by modifying the course of the entire vertebral sinusoid, accentuating or decreasing the physiological lordosis, consequently modifying the verticality of the body segments. Also in this case, a postural alteration will result.
Reduction or absence of free space: this is the opposite problem to that seen previously. In this case, the muscles placed behind the cervical spine will be activated in order to retract the head. In this way the dental arches are separated by releasing the work of the hyoid muscles. Once again, the center of gravity of the body will undergo a rearward displacement and again the underlying muscles will have to activate to maintain balance by acting on the entire spinal column by altering the verticality of the body segments. The consequence will be a postural alteration.
All the postural imbalances seen may in turn generate the onset of orthopedic pathologies (scoliosis, low back pain, neck pain, etc.) which we could define as secondary to a primary pathological involvement of the mouth apparatus.
Connection between posture and TMJ: the mechanisms seen can also act in reverse, there would be the case in which a muscle imbalance from other parts of the body causes problems in the TMJ for the mechanisms of muscular interconnection. The muscular system as a complex system can undergo primary (inherent in the system) or secondary shortenings (caused by the malfunction of other structures). In both cases there will be a postural problem over time.
Diagnosis
Posture is a complex and multifactorial problem, that is, there are many systems that can alter it (chewing, visual, auditory, neurological, musculoskeletal systems, etc.) including the emotional experience. It is the posturologist’s task to make a differential diagnosis by collaborating with various specialists for a casual as well as symptomatological resolution of the problem in question. In the specific case of the TMJ which, in percentage terms, is one of the joints most involved in postrual imbalances, the collaboration between dentist-posturologgist and physiotherapist-posturologist is necessary both in the execution of the differential diagnostic tests and subsequently in the setting of the therapeutic process. More appropriate.
It is possible to use a self-test by the patient in order to identify important elements for the diagnosis of postural pathology:
- Ear pain (in the absence of ENT problems)
- Joint noises and difficulty in opening and / or closing the mouth headache
- Cervicobrachialgia
- Lumbar and / or back pain (with head in front or behind)
Therapy
If the differential diagnosis highlights a postural problem deriving from the TMJ, the first intervention must be that of the dentist with the use of a byte or an orthotic. These (mobile) instruments preferably positioned in the lower dental arch, have the task of obtaining correct dental contact for correct swallowing and consequently correct dental positioning of the temporomandibular joint. Later, when the system has stabilized, there will be the opportunity to act stably on the teeth.
Between the byte and the orthotic, the latter is to be preferred for its precision and its characteristic of reproduce the optimal dentition.
In order to use this means, however, it is essential for the dentist to use this kinesiograph, a complex tool that allows you to model the orthotic while respecting physiological lines.
During the treatment period with the mobile device, it will also be necessary to evaluate the opportunity to support a physiotherapy treatment aimed at resolving the residual muscle shortening that has stabilized.
When, on the other hand, the differential diagnosis highlights an TMJ problem resulting from a postural imbalance, the initial work will be that of the physiotherapist-posturologist who will have to rebalance the muscular forces acting on the skeleton inn order to regain positioning physiological of all joints.
The techniques mainly used for this purpose are the Mézières Method, RPG and Rolfing. Only later, when the musculoskeletal system is sufficiently stabilized, will it be possible to evaluate the appropriateness of the dentist’s intervention with the means.
This post is also available in: Italian Chinese (Simplified)