The conservative, as the name implies, aims to preserve the tooth in its anatomical and functional integrity. The main factor that can contribute to undermining the health of the tooth is represented by caries
Caries
Caries is a microbiological disease characterized by the destruction of the hard tissues of the tooth (Fig. 1).
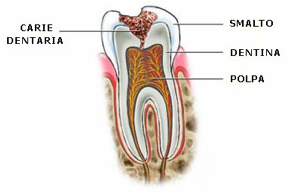
Fig.1 – Tooth decay
This is promoted by bacteria normally present in the oral cavity that digest the hard tissues of the tooth due to acids produced following the digestion of sugars ingested with the diet. In fact, it is the sugars contained in food that are metabolized by bacteria to produce acids that attack the mineralized substances (enamel and dentin) that make up the tooth and therefore cause tooth decay. There are mainly sugars such as sucrose, lactose, maltose. In addition to bacteria and sugars, there is a third determining factor in the onset of carious disease: time. In fact, it is essential that the sugars remain in contact with the tooth for a certain period of time for the demineralization process to begin. Furthermore, it has been seen that what matters is not the quantity of sugars ingested but the quality, in the sense that it is better to take a greater quantity of sugars but in a single moment rather than making small intakes of sugary foods but several times during the day. In fact, saliva contains buffer substances that serve to counteract the acidic substances produced by bacteria but, when sugars are taken repeatedly throughout the day, this buffering power cannot be successfully implemented. Anatomical factors are also important in the onset of caries. For example, the presence of particularly deep occlusal furrows and therefore difficult to clean with normal brushing, or anomalies in the formation of the enamel (such as enamel beads) which make it difficult to remove plaque. Saliva, as we have said, is also important to counteract the onset of caries. Pathologies affecting the salivary glands can have strong repercussions for the health of the teeth. Cases of hyposcialia (poos saliva production) can lead to the formation of destructive caries in short periods of time.
Classification of carious lesions
Caries begins on the surface of the tooth, occlusal or interproximal, and then continues deep into the tooth. It begins with the enamel, a highly mineralized tissue and therefore more resistant to acid attack, and then encroaches on the underlying dentin, a much “softer” tissue, where the lesion progresses much more rapidly. There may be initial lesions, hardly visible, which represent small areas of demineralization of the enamel, but which do not yet represent the actual caries. They are called “white spots” and are incipient lesions that do not require therapy but must be kept under control as they can evolve into carious lesions. The diagnosis is made by drying the surface of the tooth with a jet of air which, dehydrating the tooth, highlights these spots.
The classification divides caries according to the affected tissue and the depth of involvement of the tissues even if there are numerous classifications:
-
- Enamel caries: these are small lesions affecting the enamel of the tooth, asymptomatic, poorly visible radiographically, affecting only the tooth enamel.
- Dentin caries: they affect the enamel and dentin, but the latter is affected for less than half of its thickness. There may be discomfort with cold drinks or sugars, and they are visible radiographically.
- Advanced dentin caries: affects enamel and dentin for more than half of its thickness but there is no pulp involvement. There may be discomfort and lesions are visible radiographically.
- Advanced caries: affects enamel and dentin with pulp involvement. In this case, there is an evident symptomatology that requires the use of endodontics, and these are lesions that are clearly visible on radiographic examination.
The diagnosis is made through clinical examination and the execution of small bite-wings (they are intraoral plates that are used to identify carious lesions, especially interproximal ones).
Caries in children
Caries is a disease that affects from a young age and especially children due to their tendency to take sugars several times during the day. There is even a real pathology that takes the name of Baby Bottle Syndrome (bottle syndrome) that affects children during the first years of life (under 3 years of age during deciduous dentition) which can have serious repercussions on the development of permanent dentition (Fig. 2). It is characterized by the development of numerous carious lesions affecting almost all the dental elements of the oral cavity with a rapidly destructive course that can lead to the loss of deciduous elements at an early age. It is caused using sugary substances through the bottle during the day and especially during the night with a high frequency and without adequate cleansing after meals. Another habit not recommended is to make the baby fall asleep with a pacifier wet with sugary substances as, during the night, a reduction in salivary flow is associated which further increases the cariogenic power of sugars. Once this pathological condition has established itself, it is necessary to intervene as quickly as possible to avoid major problems. In general, attempts are made to save the deciduous elements until the eruption of the permanent elements through approximate reconstructions, given the tender age of the child who would hardly tolerate prolonged sitting in the chair.

Fig.2 – Baby Bottle Syndrome
After the eruption of the permanent elements (the first elements to erupt are the first upper and lower molars at about 6 years) it is essential to protect these very important dental elements from caries. Sealing is used, the purpose of which is to “seal” the occlusal furrows of the newly erupted molars in order to create a surface that can be easily cleaned during oral hygiene maneuvers. These are fluid resins that are deposited on the tooth surface with small brushes and hardened by means of a special light source. Sealing should be done as soon as the first molars erupt and should be checked annually. They must be replaced as soon as there are signs of deterioration.
Caries therapy
The treatment of carious lesions is based on two main phases: removal of the carious tissue and reconstruction of the tooth. Carious lesions are also classified by location, although this classification is misused. In fact, Black’s well-known classification refers to the type of residual cavity after the removal of the caries and not exactly to the site of the carious lesion. The classification is divided as follows:
- I class: cavities involving the occlusal surface of the posterior teeth (molars and premolars)
- Class II: cavities involving the interproximal surfaces of the posterior teeth (molars and premolars)
- Class III: cavities involving the anterior teeth (incisors and canines) without involvement of the incisal angle
- Class IV: cavities involving the anterior teeth (incisors and canines) with involvement of the incisal angle
- Class V: tooth neck injuries (all teeth)
The operational phases can be distinct:
- It starts with anesthesia (which can sometimes be avoided in the case of lesions confined to the enamel)
- We proceed with the isolation of the field through the rubber dam (Fig. 3). It is a device that has been used in dentistry for years. It consists of a rubber sheet perforated by the operator in the area we are interested in which is placed in the patient’s mouth to isolate the tooth that we need to treat from the rest of the mouth. In this way the operator works better as there is no presence of the tongue or saliva that hinder the dentist’s work and in addition the patient is protected from the substances that are used during the procedure. Furthermore, the materials used to reconstruct the tooth are affected by humidity.

Fig.3 – Rubber dam
- Rimozione del tessuto carioso: tramite delle frese si rimuove il tessuto carioso in modo da ottenere un substrato privo di zone di demineralizzazione. Esistono anche delle sostanze, i rivelatori di carie, basate sull’utilizzo di coloranti che impregnano il tessuto demineralizzato e favoriscono quindi la rimozione del tessuto cariato. E’ stato visto che queste sostanze spesso sovrastimano la quantità di tessuto carioso e quindi c’è il rischio di rimuovere una maggiore quantità di tessuto,anche sano.
- Ricostruzione del dente: dopo aver rimosso la carie si passa alla ricostruzione in modo da ristabilire l’anatomia originaria. Oggi si usano quasi esclusivamente i compositi, materiale bianco e quindi assolutamente estetico. Un tempo si usava molto l’amalgama, che aveva però lo svantaggio di essere grigia e inoltre, contenendo mercurio, poteva creare potenziali danni al paziente. Infatti, il mercurio contenuto nell’amalgama può essere dannoso per il paziente ma soprattutto per l’operatore. Infatti è stato dimostrato che la quantità di mercurio liberato da un’otturazione in amalgama è minimo e i rischi sono piuttosto da ascrivere al medico che, durante la sua attività lavorativa, ha posizionato centinaia di otturazioni in bocca. Il composito è presente in varie tonalità di bianco-giallo in modo da imitare il colore personale di ogni paziente. Viene portato sul dente in piccoli incrementi, modellato con strumenti appositi e infine polimerizzato con una lampada che promuove l’indurimento del materiale.
- Una volta terminata l’otturazione si procede con la rimozione della diga e la verifica occlusale
Finally, the filling is polished with brushes and abrasive pastes.
This post is also available in: Italian Chinese (Simplified)