Normally in implantology the main factor to be taken into consideration when preparing to undertake implant surgery concerns the amount of bone tissue in the site that will host the implants. If this proves insufficient, procedures are used to increase the quality. In this case, we speak of bone regeneration to describe the set of bone reconstruction techniques that are implemented in implantology when the patient does not have enough bone. This analysis is possible only after viewing a dentalscan.
Materials: The materials that can be used in bone regeneration procedures can be of autologous, synthetic or animal origin. Typically it is preferred to resort to the latter as they are accompanied by less discomfort for the patient since there is no need to remove bone from a donor site and therefore surgical trauma and postoperative discomfort are reduced. Furthermore, the scientific literature supports a higher success rate in regenerations with bone of bovine origin type BioOss which is also the one used in our center. It is bone of animal origin, typically bovine (Fig. 1 and 2), which has characteristics of absolute biocompatibility with the body, as it is subjected to special procedures during the production process that eliminate its potential allergenicity. This type of bone forms a kind of scaffolding around the implant on which the body’s bonne cells are organized and is gradually replaced by real bone. The bone harvesting from the patient himself, now in disuse, consists instead in taking it in places where it tends to be abundant (chin symphysis, upright branch of the mandible, maxillary tuber). In the past, bone was even taken from extraoral sites (iliac crest) with considerable inconvenience for the patient.

Fig.1 – bone used in implantology and bone regeneration

Fig.2 – Bovine bone in particles
Often at the same time as the bone graft, a collagenic membrane is placed that acts as a barrier for the
Newly positioned tissues so that the latter is contained in the site where it was positioned without the risk of it being moved (the so-called “curtain effect” of the membrane). These are completely resorbable membranes, so it is not necessary to remove them, and they reabsorb within a few months.
When bone regeneration procedures are performed, healing times are lengthened, passing from canonical 3 months to about 6 months.
![]()
Maxillary sinus lift
The bone regeneration procedure par excellence is represented by the maxillary sinus lift. The maxillary sinuses are two cavities present in the thickness of the upper jaw containing air and in communication with the nasal cavities through special orifices. Often after the loss of dental elements in the area of the upper molars there is a progressive thinning of the bone which, in anticipation of implant surgery, must necessarily be increased to provide adequate stability to the implants. We talk about maxillary sinus lift to indicate a particular surgical procedure that causes an increase in bone volume in the upper arch of the mouth. The term “sinus lift” is due precisely to the fact that the maxillary sinuses are moved upwards by the restoration of the bone volumes, with special materials, in order to allow a stable anchoring of the implants. The placement of the implants is done at the same time in such a way as to reduce the total time of therapy or after about 6 months from bone regeneration surgery.
Preoperative evaluation: it is necessary to have a clear picture of the general and local clinical situation of the patient, evaluating if there are any contraindications to the treatment. From a general health point of view, it is necessary to evaluate whether exist the following conditions: cardiovascular and / or respiratory decompensation, tumors, decompensated diabetes, etc. The assessment of local conditions is also important. The following pathologies affecting the maxillary sinus represent absolute contraindications to surgery: acute sinusitis, cysts, neoplasms, the presence of foreign bodies inside the sinus and periapical lesions affecting contiguous elements. However, any thickening of the sinus mucosa does not constitute a contraindication to surgery. Once this has been assessed, the intervention can be planned. In this case, the careful study of the CT scan is of fundamental importance in order to know preoperatively the amount of bone regeneration that is to be obtained from the operation.
Two raising procedures can be distinguished in: the large rise and the mini rise. In first case, the sinus is accessed from a bony window produced on the lateral surface of the sinus, while in the second, access is through the bone crest. The choice between the two techniques depends on the amount of bone to be regenerated. In fact, in the first case it is possible to obtain large bone increases while in the second these are more contained. Furthermore, the mini lift is less traumatic for the tissues and therefore causes less discomfort for the patient. Even the choice of placing the implants in the same session or at a distance of time depends on an evaluation made by the surgeon.
Surgical procedure: the “large elevation” surgery is performed with a lateral surgical access (Fig. 3). Practically, after having incised the tissues, a bony window is made on the lateral face of the sinus with the piezosurgery. After accessing the sinus, the membrane lining the inner wall of the sinus is gently lifted with special instruments. Then we proceed with the filling of the lower part of the maxillary sinus with bone substitutes. Finally, the implants are placed. Respect for the integrity of the sinus membrane is very important for the success of the operation, so it is necessary to be extremely delicate during its lifting given its fragility.
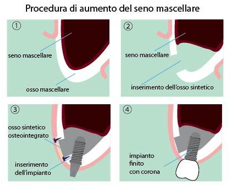
Fig.3 – Large sinus lift
The mini lift provides for access to the sinus via the crest (Fig. 4). After incising the tissues, a hole is made in the bone at the level of the edentulous crest until access to the sinus is obtained. Afterwards, the bone is inserted into the hole just made and the latter is pushed inside the sinus with specific tools. The procedure is repeated until the desired increase is obtained. When performing a sinus lift, it is possible to insert the implants at the same time or wait for a period of 7 months for the bonne to integrate with our body. Therefore, in the case of a patient who must face the elevation, it is good that he knows that the delivery time of the final prosthesis will be approximately 8-13 months from the start of therapy.
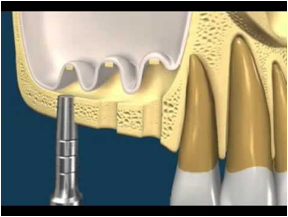
Fig.4 – Mini Sinus Lift
Complications: although the surgical technique of elevation of the sinus membrane is certainly predictable, there are not rare cases in which it is possible to encounter complications that may possibly compromise the outcome of the surgery. There may be: vascular, infections, anatomical complications linked to incomplete osseointegration. One of the most common complications is represented by the laceration of the membrane (14% of cases) of the sinus for anatomical reasons or due to inexperience. In fact, sometimes the membrane is extremely thin and fragile and therefore very easy to tear. In these cases, extreme delicacy must be used in all procedures relating to the evaluation of the membrane. If this complication is encountered, a collagen membrane is placed to prevent the bone particles from ending up in the sinus.
This post is also available in: Italian Chinese (Simplified)