Endodontics is the dental branch that deals with pulp diseases, that is, the set of vessels and nerves that are contained in the thickness of the tooth (Fig. 1). The pulp is a very cell-rich tissues and contains numerous blood vessels and nerve endings that impart sensitivity to the tooth. These structures are housed in spaces excavated inside the tooth and called pulp chamber and root canals. The vessels and nerve endings that make up the pulp tissue enter these spaces through the apical foramen, a real orifice located at the apex of the tooth. It can happen that for various reasons (for example destructive caries or dental trauma) the pulp can undergo inflammatory phenomena of varying degrees that require intervention by the specialist. Endodontics, in fact, deals with the therapy of all diseases of pulp origin.
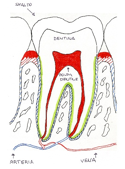
Fig.1 – Endodontal diagram
Pulp pathologies
Pulp pathologies can present with quite different pictures. Reversible pulp inflammation, irreversible inflammation and finally pulp necrosis with sensitivity to cold (for example by drinking cold water) or sensitivity to sweet foods (for example by eating a candy). It is a pain (most sensitivity) caused, in the sense that it arises only when a stimulus encounters the tooth and never spontaneously. Typically, it occurs in teeth that have carious lesions at the level of the crown and that have been neglected or following caries not visible to the naked eye (for example because they are located between one tooth and the other or in the case of “carrot” caries in the sense that they only minimally affect the tooth enamel but deepen especially in the dentin destroying it quickly). So it is always the bacteria that cause inflammation and symptoms. Generally, they do not present themselves as a form of urgency as the patient has on real pain but only a “bearable” discomfort. In this context, the pulp exhibits a moderate degree of inflammation which shows some degree of reversibility. In fact, by intervening through the treatment of carious lesions, the symptoms generally disappear. However, the situation must be monitored over time as complications can occur, in the sense that the pulp could undergo necrosis. The picture of irreversible inflammation of the pulp is different in which the tooth is especially sensitive to hot stimuli and the pain is typically spontaneous. In this case, the pulp inflammation is in an advanced stage so the only possible therapy is the devitalization of the affected tooth.
If no action is taken during this stage, there is necrosis of the tooth pulp as the toxic products of bacterial origin literally destroy the tissues. In this case the symptoms are absent as the nerve endings have been destroyed. However, there may be various symptom pictures such as abscess which is accompanied by intense painful symptoms that lead the patient to go the dentist urgently.
Even in the case of dental trauma, the pulp suffers a strong shock and over time can undergo necrosis.
It is not uncommon for a patient to o to the dentist because of a tooth that in the past has practically never bothered and which instead has undergone necrosis. This is because, at times, in the past, the patient has felt some sensitivity to a tooth but being a bearable discomfort, he did not give weight to the problem.
Symptoms of pulp diseases
Pulp pathologies are characterized by sensitivity and, depending on the case, pain. In the early stages of pulp inflammation, the only noteworthy symptom is sensitivity to cold stimuli and sweet foods. There are usually bearable symptoms. When pulp necrosis occurs, symptoms may cease instantly, but this does not mean that the situation is under control. In fact, after some time, even acute pictures such as acute apical periodontitis is characterized by sensitivity to percussion of the tooth (even when chewing) but otherwise no other relevant symptoms are to be found. In the abscess, on the other hand, in addition to the sensitivity to percussion, there is severe pain due to the pressure of the pus at the level of the periapical tissues, a sensation of “elongated tooth” and difficulty in closing the mouth. There is typically a swelling in correspondence with the affected tooth which may also be visible outside the oral cavity. Sometimes the picture of the abscess does not manifest itself but in this case a chronic inflammatory process can be established, completely asymptomatic, which takes the name of apical granuloma. It is a chronic inflammatory tissue formed by the cells of our organism that try to block the bacterial advance, and therefore circumscribe the inflammation giving life to this rounded formation. Although not accompanied by any symptoms, the granuloma over time tends to grow and turn into a cyst that must be treated as soon as possible.
Diagnosis
The diagnosis of pulpal pathologies is often simple but pictures of difficult therapeutic resolution can occur. It is essentially based on the execution of some sensitivity tests and radiographic examination.
Sensitivity test: these are designed to stimulate the pulp nerve endings to establish the health conditions of the pulp. Mainly these are thermal tests and electrical tests. Thermal tests are divided into heat tests and cold tests. The cold test is the most used to confirm the vitality of the pulp. The pulp is normally sensitive to cold but what changes inn pathological situations is the response to the stimulus. In healthy teeth, once the cold stimulus is applied to the tooth, there is an immediate discomfort which ceases soon after the cold stimulus is removed. If, on the other hand, once the stimulus has been removed, the discomfort persists, the situation is pathological, and action must be taken. The stimulus is brought to the tooth with a cotton swab soaked in a substance (ethyl chloride) which, being at a temperature well below zero, immediately stimulates the pulp nerve endings. Typically, it starts with the tooth that is least suspected in order to assess the type of reaction the patient normally has. Then the suspected tooth is examined. There is also the heat test and the electrical test but they are rarely used.
Radiographic examination: consists in the execution of a small intraoral plate performed directly in the study that serves to evaluate the conditions, not only of the tooth, but also of the periapical tissues. The radiographic examination is normal in the case of viable pulp even if compromised while it is altered in the case of pulp necrosis. When the tooth goes into necrosis, bacteria and their toxins pass into the periapical area and cause tissue destruction. Radiographically there may be nothing as in the case of an abscess or there may be a radiolucent are (darker than the rest) in the case of granuloma or cyst.
Therapy
Pulp pathologies often require emergency therapy as, often, patients come to our observation with severe pain that is often not tame with classic painkillers. The therapy is based on devitalization which consists in the removal of the infected pulp tissues and in the subsequent sealing of the canal spaces with a special material, the gutta-percha. Since patients often come to the office in urgency and therefore without a prior appointment, they resort, in the first instance, to a therapy designed to remove the pain. In a second session, by appointment, the continuation of the therapy will be provided.
Operational phases
Devitalization consists of various stages.
- Anesthesia: it is administered only in the case of a vital tooth since, if pulp necrosis has occurred, the pain does not come from the tooth (since the nerves are “dead”) but from the destruction of the periapical tissues and therefore anesthesia would not be used to eliminate pain.
- Assembly of the rubber dam: this is a device that has been used in dentistry for years. It consists of a rubber sheet perforated by the operator in the area that interests us and is placed in the patient’s oral cavity to isolate the tooth that we need to treat from the rest of the mouth. In this way the operator works better as there is no presence of the tongue or saliva that hinder the dentist’s work and in addition the patient is protected from the substances that are used during the procedure.
- Preparation of the access cavity: it consists in making a hole on the occlusal surface of the tooth with drills in order to reach the pulp chamber and identify the canal entrances. After the removal of the chamber tissues with thin instruments, the various canals are identified (we can have from 1 to 5 canals depending on the tooth).
- Cleansing and shaping of the root canal system (Fig. 2): it consists in removing and sterilizing all the pulp contents and at the same time shaping the canals. Cleansing is the main factor for the success of the therapy, as, thanks to this, the channels are disinfected from bacteria. Sodium hypochlorite is used (it is similar to bleach) which is brought inside the tooth with very fine needle syringes and is then aspirated by the assistant. This is repeated several times when cleaning the channels. At the same time, thanks to the tools used, the channels are shaped in order to have a final shape suitable for subsequent sealing. Very thin “needles” are used that are moved inside the canal to remove infected tissues and shape the canals. Today, rotating instruments are also used which have speeded up the duration of the therapy.

Fig.2 – root canal shaping
- Root canal sealing: After cleansing it is essential to seal the canals to prevent the few remaining bacteria from reproducing and causing problems again. In fact, it has been seen by numerous studies that it is impossible to achieve complete sterilization of the root canal system but only a strong reduction in the bacterial load. So, through the sealing with gutta-percha, it is as if the bacteria were “walled” alive inside the canals and therefore are destined for death (Fig. 3). For this purpose, gutta-percha is used, and orange-colored biocompatible material in the form of cones of variable diameter, which is inserted into the canal and heated to make it fluid and thus fill all the crevices of the canal system. This phase can be performed in the same session as the cleansing or in a subsequent session after about a week.
Fig.3 – Gutta-percha points
Today there is often a tendency to devitalize a tooth in single session rather than in two sessions, as was the case in the past. In fact, it has been seen that, from a success point of view, it is better to perform the therapy in a single phase. It is also true that, by performing the root canal treatment in two phases, it will be possible to better control any postoperative discomfort for the patient. Generally, the duration varies according to the treated tooth, resulting longer in the case of teeth with multiple canals (upper and lower molars) while it is faster in the case of incisors and canines (which almost always have only one canal) (Fig. 4).

Fig.4 – root canal therapy performed
Reconstruction of the endodontically treated tooth
Once the tooth has been devitalized, it must be reconstructed in order to guarantee an excellent long-term prognosis. From the world literature, it has been amply demonstrated that the best way to reconstruct an endodontically treated tooth is to cover the tooth with a prosthetic crown to prevent any fracture. In fact, devitalized teeth lose much of their strength because, being deprived of the pulp, they lose their natural hydration and therefore fracture is much more likely. Since, then, often devitalized teeth are already largely destroyed by caries, in which it is possible to reconstruct a devitalized tooth with a direct composite reconstruction or better with a composite or porcelain inlay (the difference with the filling lies in the fact that it is done in the laboratory starting from an impression and therefore it is much more precise and resistant) but only in the case in which the destruction of the tooth crown is given only by the endodontic access hole and practically all the walls of the tooth are preserved. In other cases, it is better to resort to a prosthetic crown. Furthermore, fiber posts are often used to reconstruct the core of the tooth, which has been largely demolished both by caries and by our devitalization procedures. These small white pins, made of fiberglass, are used to further reinforce the remaining tooth structure. One or more posts are placed according to the number of canals and the amount of remaining tooth substance. So, the more canals there are and the more the tooth is destroyed, the more pins are placed. Generally, a pin is sufficient in most cases. The pins are absolutely indicated in premolars (especially upper ones) as, from the literature, it has been seen that they are the teeth most subject to fracture after devitalization.
Retreatments
Sometimes it happens that a root canal therapy fails for various reasons. It may happen that a tooth has a whole series of small diameter accessory canals that are impossible to clean, or, for example, it may happen that due to obstacles inside the canals, it is impossible to properly clean the canals (Fig. 5). Or again, in the case of a therapy that went wrong because a canal was left out as a result of a previous root canal treatment undertaken by another doctor. In these cases, retreatment comes into play, the goal of which is to retreat the canals and successfully complete the therapy. It must be said right away that treatment is a much longer and more demanding therapy for the operator and the success rates are lower than a root canal therapy performed on a “virgin” tooth. In fact, it can often be difficult, if not impossible, to fully probe and clean the canals. Instruments like those used for classic root canal therapies are used but specially designed for the occasion and a solvent is used to remove the old gutta-percha.
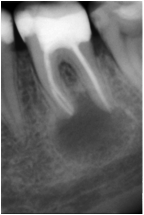
Fig.5 – Presence of lesion in an already treated tooth
Surgical endodontics
If, despite the retreatment, the therapy is unsuccessful, in the last resort, surgical endodontics, also known as retrograde endodontics, can be used. In this case, given the impossibility of obtaining therapeutic success with traditional methods, surgical removal of the apical portion of the root is used. In fact, the problem often lies in the last millimeters of the canal, where anomalies and accessory channels are typically concentrated. In practice it is a small surgery which consists of the following phases:
- Anesthesia
- Preparation of the surgical site: a flap is made at the apex of the tooth; with a bur, a hole is made in the bone and the apex of the tooth is accessed; the last 3-4 mm of the apex is cut by means of drills.
- Sealing of the canal space: after obtaining haemostasis, the site is prepared using special ultrasonic tips which are used to remove the gutta-percha from the canal for about 4 mm. Then the space created is sealed with a material, MTA, which seals and hardens in the presence of moisture.
- Execution of intraoral radiography: to verify the sealing has been completed
- Checks after two weeks, 1 month, 3 months.
This post is also available in: Italian Chinese (Simplified)