Periodontology is the dental branch that studies the tissues of the periodontium and the pathologies related to it. The periodontium consists of 4 tissues: gingiva, periodontal ligament, root cement and alveolar bone (Fig. 1).

Fig.1 – Anatomy of the periodontium
The gingiva is divided into free and adherent (macroscopically, the adherent gingiva is the one near the crown of the tooth and has a pink color while the free one is located farther from the tooth and has a darker color). Periodontal pathologies begin with inflammation of the gum and then continue in depth if no action is taken. The root cement lines the root surface of the tooth. The periodontal ligament is a kind of cushion that is located between the alveolar bone and the root cement and acts as a shock absorber during chewing. Finally, the alveolar bone is the tissue that constitutes the alveolus, i.e., the space. In which the event that the health of the tissues described above is compromised, we speak of periodontal disease (commonly called “pyorrhea”).
Incidence: periodontal disease is a very widespread disease in the world population. It is estimated that at least 10 million Italians suffer from these diseases after the age of thirty. Typically, the greatest degree of incidence occurs after the age of 50. However, there are forms of periodontal disease that arise in childhood and with an aggressive course generally of a genetic nature that lead to a rapid destruction of the supporting tissues of the tooth and require immediate intervention to prevent the loss of dental elements. Fortunately, these are extremely rare cases. It affects both genders and there are predisposing factors such as dental malposition, poor hygiene and especially cigarette smoking. Periodontal disease is a very slow but inexorable disease (in the sense that is has a continuous progression over time). It has also been shown that periodontal disease can have repercussions on the patient’s general health conditions in the presence of certain pathologies. For example, in diabetics it has been found that periodontal disease can lead to poor metabolic control of the disease. Also in patients with cardiovascular diseases (previous endocarditis or with heart valves) there is an increased incidence of cardiovascular disorders. It has also been shown that in pregnant women there is an increased risk of spontaneous abortion or premature birth or of insufficient weight of the unborn child. From all this it is clear that periodontal health is important not only locally but also to maintain normal general conditions.
Etiology: periodontal disease is caused by bacteria normally present in the bacterial plaque (these are typically anaerobic bacteria, that is, which live in the absence of oxygen) but which, in particular conditions, take over other bacterial species causing the disease. Generally, when there is a bacterial insult to the gingival tissues, and inflammatory response is generated by the body which aims to contain and resolve the attack. If the body’s defenses prevail over bacterial plaque, then a health condition is re-established. If, on the other hand, the bacterial plaque is particularly aggressive (rich in anaerobic bacteria) or the body’s defenses are deficient, then the periodontal disease continues. Therefore, the bacteria responsible for periodontal disease are those normally present in the plaque but which in particular conditions (such as poor hygiene, deficient immune defenses, etc.) take over other species and cause the destruction of the supporting tissues. In fact, it has been shown that the damage is mainly caused by the body’s defenses and not directly by bacteria.
Manifestations: Periodontal disease manifests itself with varying degrees of alterations in the normal health of the supporting tissues. It begins with localized inflammation of the gums (called gingivitis) and then continues in depth to affect the other tissues of the periodontium (bone, ligament and cement) Inn this case we speak of periodontitis (commonly called “pyorrhea”). Gingivitis manifests itself with a change in the color of the gums (which from pink to a purple red color) accompanied by bleeding (spontaneous or following brushing) and swelling. Typically there is no pain. If no action is taken, the deeper tissues are involved and are slowly but inexorably destroyed by bacteria (Fig. 2-3).

Fig.2 – Periodontal disease with significant plaque accumulation

Fig3 – Accumulatio of tartar in the lingual area
As the inflammation continues, two different pathological pictures can occur:
- Gingival recession: the gums retract and the root surface of the tooth is exposed. The teeth appear “longer” than normal and there may also be an increased sensitivity to cold due to the fact that the root of the tooth is not protected by the enamel so it becomes very sensitive. This picture is generally irreversible as the gums will no longer return to their original position unless with gingival surgery. Partial recovery can be achieved but the normal situation cannot be achieved. In this case, periodontal probing is normal. The picture typically occurs in patients with a thin gingival biotype (meaning that the gingival tissues are very thin).
- Periodontal pocket: in this case a real “pocket” is formed between the tooth and the gum which develop in depth in which anaerobic bacteria accumulate and continue the periodontal destruction. In this case, periodontal probing is pathological as a high measurement (> 4mm) is obtained by inserting the probe in the gingival sulcus. This pattern typically occurs in people with a thick gingival biotype (meaning that the gum tissues are thick).
If you do not intervene with professional hygiene sessions and possibly with smoothing then the pathology extends further leading to an involvement of furcations in the posterior teeth (furcation is the space between the roots of the teeth), increased mobility and finally loss of dental element. Typically, halitosis occurs in periodontal disease.
Quadri particolari Particular pictures
- Gingivitis gravidarum: it is a form of gingivitis that occurs during pregnancy due to hormonal production (estradiol, estriol and progesterone) typical of maternity. Gingival inflammation that originates from plaque is aggravated by these hormonal changes during the second and third trimester of pregnancy. It affects 35 to 100% of women. The gums become red and swollen. It is a picture that resolves itself after childbirth.
- Ulcer-necrotic gingivitis (Fig. 4-5): this is a particularly aggressive form of periodontitis characterized by intense pain, bleeding, rapid periodontal destruction, tissue necrosis with ulcer formation. The gums ulcerate and typically the interdental papillae are initially affected and destroyed by bacteria. Subsequently, the destruction extends to neighboring gingival tissues. After that, the tissues in depth are also involved. The course is very rapid, and it is often necessary to resort to aggressive therapies to restore a periodontal health condition even if the sequelae are typical. It typically affects developing countries due to malnutrition and consequent low-protein diet (especially children). Poor oral hygiene, poor immune defenses and especially cigarette smoking are also important factors for onset of this disease. Treatment includes oral hygiene instructions, mechanical teeth cleaning and systemic antimicrobial therapy. Furthermore, the removal of necrotic tissues is necessary.

Fig.4 – Necrotic ulcerative gingivitis

Fig.5 – Destruction of the papillae
Tobacco smoke
Tobacco smoking is a very widespread habit and cigarettes are the main product for smoking tobacco. Smoking is associated with a wide range of diseases, including stroke, coronary heart disease, peripheral arterial disease, including stroke, coronary heart disease, peripheral arterial disease, gastric ulcer and cancer of the mouth, larynx, esophagus, pancreas, bladder and cervix. It is also one of the main causes of chronic obstructive pulmonary disease and a factor associated with low birth weight of the newborn. About 50% of individuals who smoke regularly die from this habit, and smoking causes 30% of cancer deaths.
Cigarette smoke is a very complex mixture of substances, with over 4000 known constituents. These include carbon monoxide, hydrogen cyanide, oxidizing reactive radicals, a high number of carcinogens and the main psychoactive and addictive molecule, nicotine. Many of these components could modify the host’s response to periodontitis.
In studies, smokers have been shown to have higher levels of periodontitis, but associated with lower levels of oral hygiene and higher levels of tartar. Other studies have shown that smokers are more affected by periodontal disease regardless of how clean their mouth is. Summarizing the various studies and comparing smokers with non-smokers, the former present:
- Depths greater than probing and a greater number of deep pockets
- A greater loss of attachment, including a greater degree of gingival recession
- A greater loss of alveolar bone
- Greater loss of teeth
- A minor level of gingivitis and bleeding on probing
- A greater number of teeth involving furcations
The fact that smokers experience periodontal disease more frequently than non-smokers is because that smoking has on both bacterial plaque and host response.
Effects on Bacterial Plaque: Smokers may have higher plaque levels than non-tobacco users. In addition, several studies have shown that smokers have a greater number of bacterial species associated with periodontitis than non-smokers.
Effects on the host response: smoking exerts significant effects on the immune and inflammatory systems. Smokers have an increase in the number of leukocytes present in the systemic circulation but a smaller number of cells capable of migrating within the sulcus / gingival pocket. There is in fact a direct inhibition of the defensive functions of neutrophils and macrophages. It seems that smoking also affects the functionality of T and B lymphocytes, resulting in a lack of response at the functional level of T cells. Furthermore, smoking causes a reduction in all classes of antibodies except IgE.
Effects on healing and response to treatment: Smoking has been identified as an important cause of impaired healing in orthopedic surgery, plastic surgery, dental implant surgery and in all periodontal treatment modalities. In the non-surgical treatment of periodontal disease, smoking is associated with less reduction in pocket depth.
Diagnosi Diagnosis
Diagnosis in periodontology represents the first step to be able to set the right therapy. The two main tools used are: periodontal probing and radiographic examination. The probing is carried out with a blunt-tripped millimeter periodontal probe that is gently inserted into the gingival sulcus in order to obtain a measurement of the probing depth. Typically in periodontal disease there is a loss of attachment and formation of pockets for which the value in millimeters will be increased in the presence of pyorrhea. Generally values up to 3 mm are to be considered normal while from 4 mm up the situation is pathological. The probing is done for each tooth and for each tooth 3 points are examined on the external face of the tooth and 3 points for the internal one. So we will get a total of 6 measurements for each tooth examined. In fact, periodontal disease is not constantly localized on all teeth but there may be marked differences between one tooth and another and even between different points of the same tooth. The radiographic examination par excellence in periodontology is the full intraoral (Fig. 6 and 7) as it allows you to see clearly and in detail all the supporting structures of the tooth and identify pathological situations. It consists of a series of small intraoral plates (generally 18-20) that are performed directly in the office with a special equipment, and which are made in such a way as to “photograph” all the dental elements and tissues that surround them. This examination allows to detect pathologies affecting the alveolar bone surrounding the tooth.
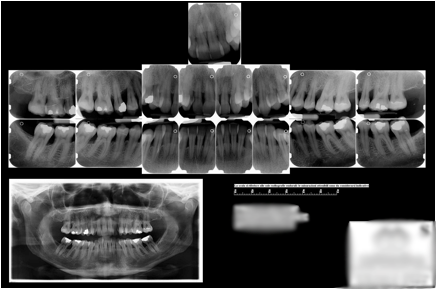
Fig.6 – full enforal
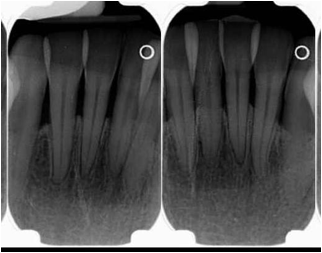
Fig.7 – detail of a plate showing bone loss at the level of the incisors
From a careful examination it is possible to obtain different pictures of increasing severity:
- Gingivitis: This diagnosis is used if one or more gum units around a particular tooth bleed during probing. There are no pockets, and the radiographic examination is normal.
- Mild periodontitis: measurement of the depth of the pockets and radiographic examination indicate a uniform loss of supporting tissues that does not exceed one third of the length of the root. There is also bleeding on probing.
- Severe (advanced) periodontitis: in this case the loss of supporting tissues that exceeds one third of the length of the root. There is bleeding on probing.
After examining the periodontal tissues, the patient’s oral hygiene must also be evaluated, recording the absence presence of plaque on each tooth surface. In addition to the plaque’s own assessments, plaque retention factors, such as supra and subgingival tartar, defective margins of dental reconstructions, etc. should also be identified and reported in the periodontal record.
Treatment
Periodontal treatment has the ultimate goal of eliminating the infection caused by bacteria and in particular the objectives to be achieved are:
- Reduction or elimination of gingivitis
- Reduction of the depth of the pockets on probing
- Elimination of furcations involved
- Aesthetics and functionality satisfactory for each patient
It can be divided into three phases: initial causal therapy (i.e., targeted to the causes and therefore removal and control of bacterial plaque), additional therapy (corrective phase) and periodontal support therapy (maintenance therapy).
Initial causal therapy: aims to remove or control the infection caused by plaque and consists of:
- Instructions on oral hygiene
- Scaling and root smoothing
- Reconstruction of carious lesions
- Any endodontic therapies
- Any extractions
The first phase of causal therapy consists in scaling or ablation of supra and subgingival tartar (Fig. 8). It is practiced with ultrasonic instruments capable of breaking up the bacterial film and tartar from the surface of the teeth. The instrument, thanks to the liquid that is activated by ultrasound, leads to an excellent elimination of tartar and plaque. There may be sensitivity during treatment and immediately after it subsides within a few days. This is since once the tartar has been removed from the tooth surfaces, the root surface of the tooth is exposed, which is therefore sensitive. The session lasts about an hour and after that you immediately feel a cleansing sensation in the oral cavity. In the first session the oral hygiene instructions are also explained.

Fig.8 – Scaling
In the event that the presence of periodontal pockets was already found during probing, after the first scaling session, we will proceed to the phase of root planning or scaling (Fig. 9). Root planing consists in “scratching” the root surface of the tooth with tools called curettes which are inserted into the periodontal pocket and remove tartar and plaque from the root surface of the tooth. They also remove the inflammatory tissue that makes up the pocket. The polishing sessions are divided into 4 appointments during which a quadrant of the mouth is treated for each session (right upper half arch, left upper half arch, right lower half arch and left lower half arch). Each session lasts about 45 minutes. The smoothings are performed under local anesthesia and post-therapy discomfort is generally minimal or nil.
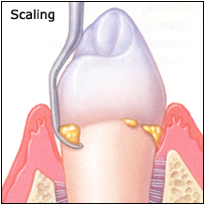
Fig.9 – Root planing
After the first phase of therapy, it is necessary to wait about two months before proceeding with a re-evaluation of the periodontal situation. In most cases, if the patient strictly follows the oral hygiene instructions, the disease can be kept under control without further problems. However, it is necessary for the patient to undergo periodic follow-up and maintenance visits.
If the desired results do not accomplish, it is possible to proceed to the second phase of the therapy (corrective phase): we will proceed to the extraction of the elements that can no longer be stored, to an additional endodontic treatment, to periodontal surgery (only in those areas in which scaling, and root planning procedures had no effect), upon insertion of dental implants. Periodontal surgery includes a whole series of surgical procedures aimed at the removal of inflamed tissue and the re-establishment of anatomical conditions that disadvantage the accumulation of plaque.
Once initial therapy and adjunctive therapy have been completed, the patient should undergo recall visits (maintenance therapy) to prevent any recurrence of the disease. These visits are generally scheduled every 3-4 months. During these recall visits the following should be performed: evaluation of the standard of oral hygiene and mechanical removal of tartar with polishing of the teeth.
Plaque self-control
As has been widely said, plaque is the main cause of periodontal disease and therefore the techniques to remove it are the most important factor to prevent the onset of the disease and, once established, to prevent its progression. The procedures implemented to control plaque are essentially two: the use of toothbrush (Fig. 10) and dental floss. The effective removal of plaque associated with the use of the toothbrush is due to three main factors: shape of the toothbrush, the ability of everyone to use the toothbrush, frequency and duration of use of the toothbrush. It is absolutely not recommended to use the toothbrush with the horizontal technique and for a duration of less than two minutes.

Fig.10 – The toothbrush must be used at least 2 times a day for about 2 minutes
An ideal toothbrush should have the following characteristics:
- Dimensions of the handle suitable for the age and skill of the user
- Dimensions of the head conform to those of the patient’s mouth
- Use of nylon or polyester filaments with rounded ends and a diameter not exceeding 0.23mm
- Using soft bristle configurations
- How to arrange the bristles that facilitate the removal of plaque in the interdental spaces and along the gum line
The recommended brushing technique is also called “from red to white”: practically you must position the toothbrush at 45 degrees towards the gum surface (the red) and rotate it gently towards the tooth (the white). This must be repeated for each tooth and on the inner surface of the tooth. Brushing must obviously also affect the occlusal surfaces of the teeth. The duration must be at least 2 minutes at least twice a day. The toothbrush needs to be replaced when the bristles begin to bend regardless of the time of use. Electric toothbrushes represent a valid alternative especially for the handicapped and for people with little manual dexterity. Studies have shown that an electric toothbrush removes more plaque than a manual one for the same brushing time. However, just brushing the teeth is not sufficient to effectively control the interdental plaque, so it is necessary to use dental floss (Fig. 11). The floss, if used correctly, can remove up to 80% of the interdental plaque and of the subgingival plaque as it can be introduced up to 3 mm below the visible tip of the papilla. It is present in a waxed and non-waxed version but there is no difference in the ability to remove plaque.
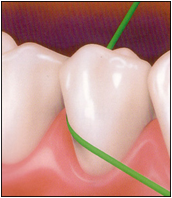
Fig.11 – Dental floss
Another way for the removal of interdental plaque is the interproximal brush (called interdental brush) available in various sizes distinguished by a different color of the handle (Fig. 12). They must be chosen in such a way as to adapt as much as possible to the interdental spaces of everyone. They represent the ideal instrument when the interdental spaces are sufficiently “open” in which the root surfaces have concavities or grooves or in the case of furcation defects from side to side or below dental bridges.

Fig.12 – Interdental brush
Additional aids: These include dental irrigation devices, lingual scrapers and toothpastes. The former devices are designed to remove plaque through the mechanical action of a jet of water. They are particularly useful in the presence of fixed bridges or orthodontic appliances that make it difficult to use the interdental cleaning devices correctly. The back of the tongue contains many microorganisms that can spread to other parts of the oral cavity. For this reason, it has been argued that lingual brushing should be part of daily home oral hygiene as it can contribute to the reduction of what is considered a potential reservoir of microorganisms that contribute to plaque formation. Furthermore, bad breath can originate from bacterial deposits on the back of the tongue. Therefore, the use of lingual scrapers should be recommended. Finally, the toothpaste is commonly used together with the toothbrush to facilitate the removal of plaque and to apply chemical agents for therapeutic and preventive purposes on the surface of the teeth. For example, the addition of abrasive substances simplifies the removal of plaque and surface stains. In the toothpastes present on the market, fluorides are commonly present with the primary purpose of preventing tooth decay. There are toothpastes containing antibacterial (triclosan) and antitartar (pyrophosphates) substances.
Effects and Consequences of Incorrect Use of Mechanical Plaque Removal Devices: There is a potential for harmful effects related to these oral hygiene practices. Brushing can cause damage to both hard and soft tissues. Soft tissue trauma causes gingival recession, while hard tissue trauma leads to cervical abrasion of the tooth surface. These injuries are related to the stiffness of the toothbrush, the method and the frequency of brushing. Cervical tooth abrasion is typically caused by brushing conducted with exaggerated pressure. Associated with tooth abrasion, gum recession often occurs, generally due to the brushing method (horizontal brushing method). Even the use of dental floss, interdental brushes and toothpicks can damage soft tissues, but these are often acute injuries, such as laceration and gum erosions.
Additional aids: these include dental irrigation devices, lingual scrapers and toothpastes. The former devices are designed to remove plaque through the mechanical action of a jet of water. They are particularly useful in the presence of fixed bridges or orthodontic appliances that make it difficult to use the interdental cleaning devices correctly. The back of the tongue contains many microorganisms that can spread to other parts of the oral cavity. For this reason, it has been arguing that lingual brushing should be part of daily home oral hygiene as it can contribute to the reduction of what is considered a potential reservoir of microorganisms that contribute to plaque formation. Furthermore, bad breath can originate from bacterial deposits on the back of the tongue. Therefore, the use of lingual scrapers should be recommended. Finally, the toothpaste is commonly used together with the toothbrush to facilitate the removal of plaque and to apply chemical agents for therapeutic and preventive purposes on the surface of the teeth. For example, the addition of abrasive substances simplifies the removal of plaque and surface stains. In the toothpastes present on the market, fluorides are commonly present with the primary purpose of preventing tooth decay. There are toothpastes containing antibacterial (triclosan) and antitartar (pyrophosphates) substances.
Effects and Consequences of Incorrect Use of Mechanical Plaque Removal Devices: There is a possibility of adverse effects depending on these oral hygiene practices. Brushing can cause damage to both hard and soft tissues. Soft tissue trauma causes gingival recession, while hard tissue trauma leads to cervical abrasion of the tooth surface. These injuries are related to the stiffness of the toothbrush, the method and the frequency of brushing. Cervical tooth abrasion is typically caused by brushing conducted with exaggerated pressure. Associated with tooth abrasion, gingival recession often occurs, generally due to the brushing method (horizontal brushing method). Even the use of dental floss, interdental brushes and toothpicks can damage soft tissues, but these are often acute injuries, such as lacerations and gum erosions.
This post is also available in: Italian Chinese (Simplified)